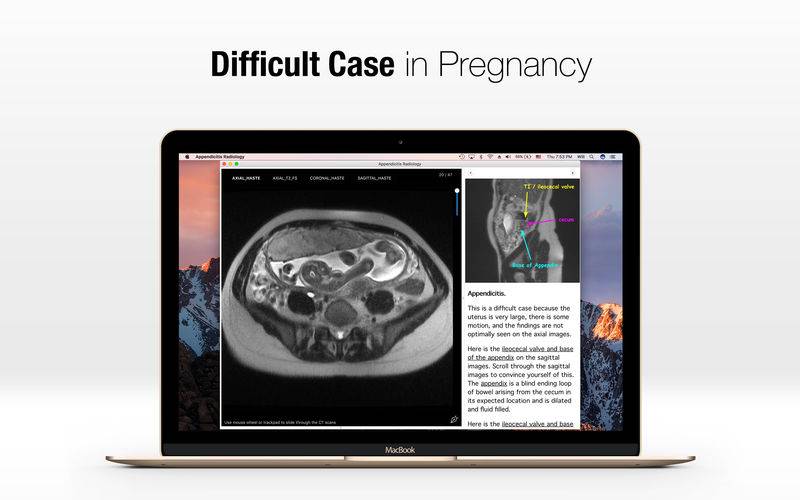
Acute appendicitis is the most common general surgical problem encountered during pregnancy. The diagnosis is particularly challenging during pregnancy because of the relatively high prevalence of abdominal/gastrointestinal discomfort, anatomic changes related to the enlarged uterus, and the physiologic leukocytosis of pregnancy.
Now learn how to diagnose Appendicitis in pregnancy, with real world MRI cases here.
Appendiceal rupture occurs more frequently in pregnant women, especially in the third trimester, possibly because these challenges and reluctance to operate on pregnant women delay diagnosis and treatment.
Acute appendicitis is suspected in 1/600 to 1/1000 pregnancies and confirmed in 1/800 to 1/1500 pregnancies. In a case control study of 53,000 women undergoing appendectomy, pregnant women were less likely to have appendicitis than age-matched, nonpregnant women. The incidence of appendicitis was slightly higher in the second trimester than in the first and third trimesters or postpartum. In addition, cohort study of over 350,000 pregnancies reported that the rate of acute appendicitis was 35 percent lower during the antepartum period than the time outside of pregnancy. This study reported the lowest rates of appendicitis during the third trimester. For women aged 15 to 34 years, there was no increased risk in postpartum appendicitis compared with the time outside of pregnancy. In contrast, an 84 percent increased risk of postpartum appendicitis was reported for women older than 35 years.
Patient presentation — In the "classic" presentation, the patient describes the onset of abdominal pain as the first symptom. The pain is periumbilical initially and then migrates to the right lower quadrant as the inflammatory process progresses. Anorexia, nausea and vomiting, if present, follow the onset of pain. Fever up to 101.0ºF (38.3ºC) and leukocytosis develop later.
However, many patients have a nonclassical presentation, with symptoms such as heartburn, bowel irregularity, flatulence, malaise, or diarrhea. If the appendix is retrocecal, patients often complain of a dull ache in the right lower quadrant rather than localized tenderness. Rectal or vaginal examination in such patients is more likely to elicit pain than abdominal examination. A pelvic appendix can cause tenderness below McBurney's point (described below); these patients often complain of urinary frequency and dysuria or rectal symptoms, such as tenesmus and diarrhea. The spectrum of clinical and laboratory findings associated with acute appendicitis is described in detail separately. (See "Acute appendicitis in adults: Clinical manifestations and differential diagnosis".)
Pregnant women are less likely to have a classic presentation of appendicitis than nonpregnant women, especially in late pregnancy. The most common symptom of appendicitis, ie, right lower quadrant pain, occurs close to McBurney's point in the majority of pregnant women, regardless of the stage of pregnancy; however, the location of the appendix migrates a few centimeters cephalad with the enlarging uterus, so in the third trimester, pain may localize to the mid or even the upper right side of the abdomen.